As COVID-19 cases become more prevalent in the general population, you may need to understand the available treatments. From a public health perspective, prevention is preferred over treatment so it is still important to continue masking, maintaining distance from others, and staying up to date with vaccinations.
Around 80% of the population have mild symptoms and can recover safely at home.
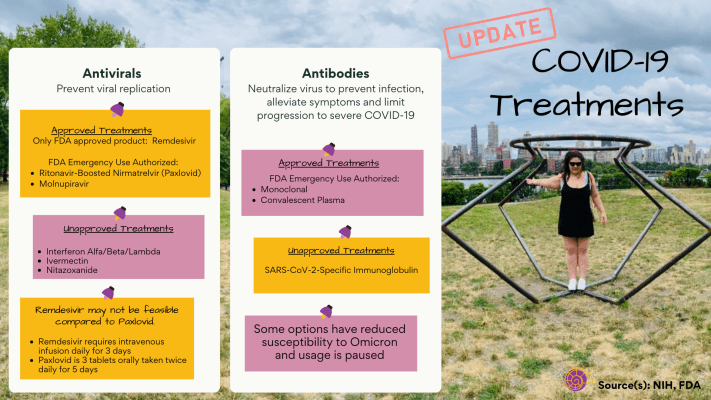
If you have moderate or severe symptoms, your treatment will depend on clinical efficacy, availability, feasibility of administering, drug interactions, and which variants are most prevalent in your neighborhood.
In December 2021, the FDA re-issued a warning that Ivermectin currently has insufficient evidence for treatment of COVID-19. Ivermectin is still under investigation in clinical trials, but currently the NIH cites a total of 9 clinical studies that show no improvement in symptoms, and no differences in mortality or hospital length of stay.
FDA Emergency Use Authorized Monoclonal Antibodies include: Bamlanivimab plus Etesevimab*; Bebtelovimab OR Casirivimab plus Imdevimab*, Sotrovimab*, Tixagevimab Plus Cilgavimab (* means paused due to reduced Omicron susceptibility).
For non-hospitalized patient, antiviral therapy is recommended (Paxlovid preferred over Remdesivir). If those are not available/feasible/clinically appropriate, use antiviral Molnupiravir or antibody Bebtelovimab.
Hospitalized patients are given Remdesivir as it needs to be administered with an IV over a period of three days.
As you may have heard, Biden recently approved at-home tests for households delivered by USPS. As we increasingly face COVID-19 testing situations, we will talk about which test is appropriate for when and what it tells you.
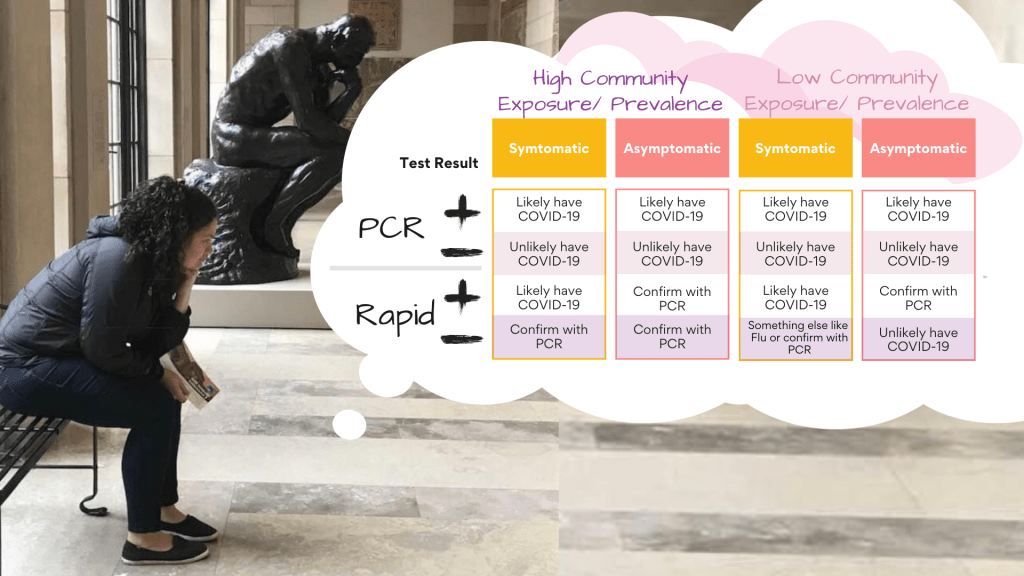
The PCR test is more accurate than the rapid antigen test. PCR tests are also known as nucleic acid amplification tests that amplify the sample through making copies to ensure better detection. Tests that have multiple virus gene targets are less susceptible to errors detecting variants.
A positive result for diagnostic tests indicates the presence of the virus spike protein for the rapid antigen test or the virus’ genetic makeup for the PCR test. Cross-contamination or sample mix-ups can cause false positives. Poor sample collection can cause false negatives.
High community prevalence or exposure increases your chance of testing positive and gives a sense of how likely your positive result is true.
Having symptoms is an indication that you may be infected, but being asymptomatic does not mean you are not infected nor does it mean your viral load is lower than someone who is symptomatic.
The PCR test is the most accurate diagnostic test. The rapid antigen test can provide a quicker diagnostic result and is available at-home, however it is less accurate and interpretation is dependent on whether you are symptomatic and in a community of high prevalence or have high exposure.
The impacts on health in early life cumulatively influences the next stages all the way through old age. The life course model allows us to visualize new life choices within the context of COVID-19 (summary table at the bottom).
Fetal/Infant
Everyone is affected including persons not yet born and those in early life. The stress felt by pregnant women and expectant fathers translate in utero and can lead to premature births. Additionally, fathers may be more involved with young children because of the shift to at-home work which benefits young children. However, toddlers are sensitive to changes that they cannot yet understand and will need to be monitored to prevent lasting negative health effects.
Childhood
Children tend to develop anxiety in seeing parents distressed in tandem with an introduction of new social rules about dangers that they cannot see. Children may experience lasting scars from poor nutrition, anxiety, family instability, domestic violence since they are undergoing stress during pivotal times in development.
Adolescent and Young Adulthood
Adolescents and young adults may be more prone to PTSD diagnoses in the future due to excessive screen exposure prompted by the pandemic. Additionally, they may experience forgone educational opportunities limiting their ability to succeed in future endeavors.
Young adults are often blamed for disregarding protective measures. Furthermore, young adults may experience difficulty gaining work experience and never catch up to earlier cohorts in socio-economic attainment which ultimately leads to poorer health outcomes.
Adulthood
Adulthood career and family formation are disrupted. This adds “insult to injury” for millennials in their thirties who went through the 2008 recession. Relationships at this stage are at risk–partnerships may be difficult to form and sustain. Additionally, excess stress has been put on women of working age to support themselves, their families, potentially newborns; all of which they may have to tackle alone.
Elderly
The Elderly are faced with increased instances of discrimination and loneliness as they may be forced into permanent retirement. COVID-19 protocols have required many people of old age to say goodbye from a distance and die alone. They may opt to age in place instead of at elderly centers because these places have become high risk for contracting COVID-19, especially when they are more likely to develop a severe case. At this stage, more elderly have shown a greater value for positive and meaningful life experiences due to these dire circumstances.
Lifetime/Cumulative
The pandemic has underscored the reality that life’s choices are limited. Cohorts may never catch up to earlier and later cohorts; have continuing disadvantages that lead to poor health outcomes later in life. Markets have stagnated and people may be stranded away from loved ones due to travel restrictions.
The lasting effects of outliving a partner, child, or loved ones who died from COVID-19 destabilizes mental health. However, the pandemic has highlighted existing inequity and led to more instances of the use of collective action to address systemic racism. The cumulative effects of COVID-19 requires that we address the weaknesses in our social systems. The life course model allows us to acknowledge intervention points at each life stage to help us all work toward a healthier future.
COVID-19 CRISIS
Health
Personal Control & Planning
Social Relationships & Family
Education & Training
Work and Careers
Migration & Mobility
Fetal/Infant
The stress felt by pregnant women and expectant fathers translates in utero and can lead to premature births
–
Fathers more involved; toddlers sensitive to changes that are not understood
–
–
–
Childhood
Lasting scars from poor nutrition, anxiety, family instability, domestic violence; excessive screen exposure can lead to PTSD
–
–
Amount/lack of resources affects remote learning quality
–
–
Adolescent
High unemployment rates and greater health risk as “Gig Economy” workers
Maybe blamed for disregarding protective measures
Difficulty gaining work experience
Delayed educational transitions and adulthood in navigating labor, housing and relationships
Cumulative impact from loss of training, experience and promotion
Postponed or forgone education abroad or career moves
Adulthood
Disruption and delayed care
Increased burden from supporting relatives how may not be settled in employment and housing
Postponement of partnering or accelerated separation; child delivery/birth alone; maybe thrusted into a caregiver role
Long-term earning negatively impacted for those entering workforce
Labor market exclusion; “lost generation” with truncated career and family formation; adding “insult to injury” for cohort in thirties who went through 2008 recession
Families left behind by seasonal workers
Old Age
Higher risk for severe COVID-19
Optimize positive and meaningful experiences
Dying alone or saying goodbye from a distance
–
Ageism and forcing permanent retirement
Aging in place instead of elderly centers that have become high risk for COVID-19
Lifetime/ cumulative
Cohorts may never catch up to earlier and later cohorts; have continuing disadvantages that lead to poor health outcomes later in life
Using collective agency to address systemic racism when individual control loss
Outliving partner or child who died from COVID-19
More openness and responsiveness for ongoing education
Career inequalities; fewer “weak/bridge ties” lessen employment opportunities
Limited migration, stranded and less globalization of labor markets
Updated on April 27th, 2021 with summary table on how common COVID-19 vaccine concerns are addressed and their sources at the bottom.
By Michelle Rufrano & Jean-Ezra Yeung
Executive Summary
Multiple COVID-19 vaccine surveys show that the plan to get the vaccine is about half of the U.S. population, and Blacks showed the highest level of concern
Contemporary racism is compromising vaccine access for communities of color
Clinical trials should adapt representation to accommodate the highest burden of disease
This includes any under-represented group (e.g. age, gender identity, ability, immigrant status, etc.)
The surveys show that the top concern is side effects
Some vaccine concerns were unfounded (acquiring infection from vaccine and costs) from mis/dis-information, but others reflect a fundamental mistrust
Many articles have heavily leaned on historic racism as way to explain away the presence of vaccine hesitancy in communities of color, but action can only be taken if we address the ways racism is expressed today. Black and Brown Americans are the most distrustful of the vaccine, yet they are also have the highest mortality and morbidity ratesdue to the coronavirus itself. Contemporary racism, therefore, manifests in cultivating an environment where communities of color distrust something that they need more than any other group.
This phenomenon is supported across four COVID-19 vaccine surveys (see summary table at the bottom) and clinical trial data. The survey data shows that only about half of the U.S. population is planning on getting vaccinated — Blacks have the strongest level of concern. Across all groups, the top concern is side effects, which have been documented in sizable proportions from clinical trials. Most of the other concerns can be categorized as mis/dis-information, and mistrust in medical research, development and practice. The clinical trials conducted by Pfizer-BioNTech, Moderna, and Johnson & Johnson’s Janssen all mirror lack of representation in recruitment of study participants. Under-represented groups are rightfully nervous about getting a vaccine if people with their specific social identities are not adequately included at the research stage.
This phenomenon is known as the “Tuskegee effect” or the lingering distrust of participation in medical trials aptly named by a one of the most well-known historic disregard for black male health specifically needs to be addressed. Furthermore, acknowledgement of how racism manifests today is tantamount to helping people of all backgrounds access care. The COVID-19 pandemic shows us how a disproportionate impact on a subgroup affects everyone in the (global) community, alongside dire strains on (public) health systems. Consequently, clinical trials and public health efforts should adapt representation to accommodate those with the highest burden of disease.
The decision to get vaccinated or individuals who got vaccinated is split around the middle
47% plan to get the vaccine
51% plan to get the vaccine if they haven’t yet
55% received at least one dose
Half of U.S. plan to get the vaccine, if they haven’t already
There are racial differences, specifically Blacks had a stronger level of concern and there was a lack of confidence that there was adequate testing on their race/ethnicity
Blacks (24%) are less likely to plan to get the vaccine than Whites (53%) and Hispanics (34%)
Non-Hispanic Blacks (30%) are least likely to plan to get the vaccine compared to Hispanics (47%), Non-Hispanic Whites (56%), and non-Hispanic Asians (66%)
Vaccine enthusiasm is higher in Whites (61%) than in Hispanics (52%) and Blacks (41%)
Half of Blacks (50%) and one third of Hispanics (34%) were not confident the vaccine was adequately tested on their race/ethnicity
Blacks (61%) are the least likely to plan to get the vaccine or already did compared to White (69%), Hispanic (70%), and Asians (91%)
Yet Blacks expressed a higher level of concern about the pandemic across six questions, such as getting infected and being hospitalized or knowing someone that did
Blacks expressed less confidence in the vaccine research and development process
There are myriad vaccine concerns and side effects is at the top of the list*
The top reason for not getting the vaccine or being unsure are side effects (71%), development/approval process (57%), infection from the vaccine (37%)
The top concerns were side effects (51.2%) and plan to wait and see if it is safe (50%)
The top concern is side effects (56%), followed by out-of-pocket costs (35%), missed work from side effects (34%), get COVID-19 from vaccine (33%) and won’t be able to get it at a trusted place (30%)
The major reason is side effects (72%), vaccine developed too quickly (67%), want to know more how they work (61%), seen too many medical system mistakes in the past (46%), don’t need it (42%), and don’t get vaccines in general (36%)
*Some of the concerns are unfounded, such as out-of-pocket costs (only for the vaccine, not the administration if not the only service in visit) and getting the infection.
Note: I would say the KFF and Pew Center Research surveys were the most comprehensive, if you wanted to look at them in more detail.
Updated on April 27th, 2021 with summary table on how common COVID-19 vaccine concerns are addressed and their sources:
Concern
Answer
Source
Side effects
In clinical trials, the most common side effects (>50%) were at the injection site (e.g. pain) and others (>~40%) include fatigue, fever, muscle pain, headache. Allergies were reported. Rare events occurred but were not related.
FDA, NEJM, NIH clinicaltrials.gov (see bottom of table for links)
Vaccine development and approval process
Research, development and approval were accelerated from: genetic sequencing technology and sharing; existing coronavirus research; no financial risk from US government’s Operation Warp Speed funds; ease of participant recruitment; and Emergency Use Authorization
Pfizer-BioNTech, Moderna and Johnson & Johnson’s Janssen vaccines (mRNA or viral vector) do not use the COVID-19 virus, but they help generate the spike protein that triggers antibody and immune responses against COVID-19.
The vaccine and its administration in a visit without other services should be covered by insurance (providers can request administration reimbursement from the government for uninsured). Certain states passed law to give employees hours aside from sick time to get the vaccine (e.g. New York State on March 21 for 4 hours per vaccine dose).
People haven’t viewed doctors and medical researchers as trustworthy when it comes to transparency and responsibility. Also for healthcare providers, people felt rushed and confused about instructions.
The UK, South African and Brazilian variants are of concern because of increased prevalence and they carry mutation(s) such that vaccine and antibody therapies have shown less neutralizing activity in the lab
Early Novavax clinical trial findings showed lower vaccine efficacy against the South African variant compared to the UK variant
The New York variant is of concern because of increased prevalence and it carries a mutation (like the South African variant) where vaccine and antibody therapies have shown less neutralizing activity in the lab
—
My first blog post was about whether the vaccines would address variants and I noted that scientists needed to do more research. Some of that research is now suggesting how current vaccines could be less effective against variants if they carry specific mutations.
I started out trying to understand how variants are defined and there are three nomenclatures. I will use the PANGO lineage here since it is the most detailed and can help track emerging variants (the other two are GISAID and Nextstrain).
In the media, you may have heard about the UK (B.1.1.7), South African (B.1.351) or Brazilian (P.1) variants of concern, but these are not technical terms (I’ve put the PANGO lineage in parentheses). These are variants of concern because of increased prevalence and they carry mutations where vaccine and antibody therapies have shown less neutralizing activity in the lab. Furthermore, the South African variant (versus the UK variant) showed lower efficacy in preliminary findings of the Novavax vaccine study. In America, the New York variant (B.1.526) is currently a variant of concern because it showed increased prevalence and was reported as the carrying the mutation (E484K) where vaccine and antibody therapies showed less neutralizing activity in the lab.
All three vaccines (Pfizer-BioNTech, Moderna, Johnson & Johnson’s Janssen) were developed based on the Wuhan variant.
Although the efficacy rates appeared lower in Johnson & Johnson’s Janssen vaccine, it was tested on a more diverse demographic population (race, more participants with co-existing conditions) and geography (including South America, South Africa), and also at a later date range (closer to the fall rather than spring/summer) such that variants could have been more pervasive.
In the studies, it is common (>50%) to experience injection site adverse events such as pain
Other common (>~40%) adverse events include fatigue, fever, mylagia (pain in the muscle), headache
Allergies were reported during or after studies
The only clear advantageous of Johnson & Johnson’s Janssen vaccine is that it administered as one shot versus two for the other vaccines
—
When the Johnson & Johnson (J&J) vaccine first came out in America, the television news I watched reported a lower efficacy rate (than the Pfizer-BioNTech and Moderna vaccines) but it had been tested for use in a more diverse demographic population and geography. At first glance, it sounded like the J&J vaccine would be better since it might address variants (J&J is advantageous logistically for only being one shot versus two for the other vaccines). Last week, I was asked by readers about the comparison between the vaccines. I’ve neatly summarized the key pieces of information in a table at the bottom (information was extracted from the FDA, NIH and New England Journal of Medicine).
The key notes from the table are as follows:
The Pfizer and Moderna vaccine trials included predominantly White and US-based participants, whereas J&J was markedly more diverse in race and country (59% White and just under half are US-based)
All three vaccines were developed from the strain found in Wuhan, China around January 2020
Adverse events (AE) were similar across vaccines
Local AE around the injection site, such as pain, swelling
Top systemic AE were fatigue, headache, mylagia (pain in muscles), fever
Serious AE were reported but not concluded as vaccine related
Allergies were reported during or after study
Primary efficacy endpoints were similar: COVID-19 diagnosis determination by PCR test with symptoms 7 or 14 days after last dose
22.5% (page 17) were at risk for severe COVID-19 at screening (had at least one of the interested risk factors)
59% White, 19% Black/African American (45% Hispanic/Latino)
~34% aged 60+
~40% (page 18) have co-morbidities that risk progression to severe/critical COVID-19
Countries
76.7% US, 15.3% Argentina
US only
Top 3 countries: US (~47%), Brazil, South Africa (others: Argentina, Chile, Colombia, Mexico, Peru)
Strain
The development was initiated on January 10, 2020, when the SARS-CoV-2 genetic sequence was released by the Chinese Center for Disease Control and Prevention and disseminated globally by the GISAID (Global Initiative on Sharing All Influenza Data) initiative
Shortly after the SARS-CoV-2 genetic sequence was determined in January 2020, mRNA vaccine was developed by Moderna and the Vaccine Research Center at the National Institute of Allergy and Infectious Diseases (NIAID), within the National Institutes of Health (NIH)
The vaccine was derived from the Wuhan strain (Wuhan 2019; whole genome sequence, NC_045512)
Participant country/variant analysis (71.7% sequenced as of February 12, 2021): US (96.4% Wuhan D614G variant), South Africa (94.5% B.1.351 lineage), Brazil (69.4% P.2 lineage, Wuhan D614G variant 30.6%); B1.1.7 and P.1 lineages were not found
At least 78% reported pain locally (at injection site) after either dose for aged under 56; aged 56+ was at least 66%
At least 42% or 48% reported headache or fatigue respectively after either dose for aged under 56; aged 56+ was at least 25% or 34% respectively
Unsolicited adverse events up to 30 days after vaccine: 0.4% percent in under aged 56 reported serious adverse events; aged 56+ was 0.8%; non-serious was 29.3% n under aged 56; aged 56+ was 23.8%
Allergic reactions were voluntarily reported post-authorization/trial
86% reported pain at injection site.
Top systemic were fatigue, headache, myalgia (pain in muscles). 54.9% of any event after first dose and 79.4% after second.
23.9% of participants reported unsolicited adverse events 28 days following each vaccine (as of November 25, 2020)
Allergic reactions are possible
Solicited local (where injection occurred): 59.6% reported pain aged 18-59; 33.3% over aged 60
Top systemic (headache, fever, myalgia – pain in muscles): 39-44% aged 18-59; 24-30% over aged 60
Unsolicited 28 days after vaccination: none with causal relation to J&J (13.1% versus 12% in vaccine versus placebo group) as of January 22, 2021.
Allergic reactions were reported during study
Primary Endpoint & Efficacy
95%; Primary efficacy analysis is no infection 7 days after 2nd dose without prior infection (COVID-19 determined by RT-PCR test and at least 1 related symptom)
94.1%; Primary efficacy is positive RT-PCR test and at least two systemic or at least on respiratory symptom 14 days after second injection
End points are moderate to severe/critical COVID-19 using PCR test and symptoms at 14 and 28 days after vaccination (66.9%, 66.1% efficacies), for severe/critical (76.7%, 85.4% efficacies). Percentages varied by country (lowest rates in South Africa).
Updated on May 13th, 2021 with summary table on COVID-19 tests and their sources at the bottom.
Executive summary
A diagnostic test directly affirms the presence of the COVID-19 virus
Rapid (molecular), antigen and antibody tests were deployed for more widespread testing at a lower cost to develop baseline infection rates, especially in outbreak or congregate settings, such as nursing homes and schools. They maybe less accurate than the diagnostic test
If you have symptoms or COVID-19 exposure, it is recommended you get a diagnostic test
—
Quite quickly, the different types of COVID-19 tests caused me confusion as to which one I would need and when. In New York City, there is a one-size-fits-all message to get tested. It is recommended by the Test & Trace Corps (published January 6, 2021) to get tested immediately if you have symptoms or (possible) exposure, and periodically if you work outside of your home. However, it is still not clear which test you should get.
The antigen test is recommended (published October 17, 2020) in New York State for use in congregate settings like nursing homes and schools. It is relatively less expensive but less sensitive than a diagnostic test. However, there are recommendations to get the diagnostic test as a confirmation of a positive result. A rapid molecular test was also developed to be used in contexts like nursing homes and schools, similar to the antigen test, and it also recommends a confirmatory diagnostic test for positive results.
New York State uses the antibody test to develop a baseline infection rate. The test developed by the state detects antibodies in the blood, specifically IgG, which is usually developed three to four weeks after infection. It is not recommended to take this test until twenty-one days after a positive diagnostic test or the symptoms of COVID-19 started. Only the diagnostic testitself detects the virus’ genetic makeup.
Updated on May 13th, 2021 with summary table on COVID-19 tests and their sources.
Diagnostic, detects spike protein on virus’ surface
Non-diagnostic, detects antibodies fighting against virus
Use
Most accurate for current infection
Less accurate but more affordable for current infection
Check for prior infection (requires 1-3 weeks after infection)
Scenario
Known exposure or symptoms; lab version to confirm less accurate test (positive, or symptomatic but negative test from antigen or non-laboratory version)
Known exposure or symptoms; high-risk congregate settings; routine screening
If you have Commercial (non-grandfathered, non-self-funded), Medicare Advantage or Medicaid, insurers have been waiving cost-sharing for COVID-19 treatment (the largest insurers so far have set time frames and extensions until at least end of 2020)
If you are on traditional Medicare or in a Commercial Obamacare-compliant health plan and do not have cost-sharing waived, you may have to pay out-of-pocket.
Pneumonia has been used to estimate out-of-pocket costs and this could start at $1,300 depending on complications (e.g. ventilator usage), deductible amount based plan type (large group, small business, individual); and balance/surprise billing is estimated to occur for one in five cases
If you are uninsured, the Provider Relief Fund can reimburse your provider if they apply for it
—
The American media has heavily focused on coverage and accessibility to COVID-19 testing and vaccines, but I saw little coverage on COVID-19 treatment should you unfortunately need it. I looked into what it might cost you out-of-pocket for the entire treatment.
The Kaiser Family Foundation laid out how traditional Medicare would cover hospital stays but beneficiaries would need to pay deductibles ($1,484), whereas it is recommended for Medicare Advantage plans to waive cost-sharing. They also projected COVID-19 hospital cost using historical claims on pneumonia for private (employer-sponsored) health insurance (published March 13, 2020). They estimate out-of-pocket costs exceeding $1,300 but private insurers have been waiving cost-sharing requirements so far. Medicaid patients have no cost-sharing for COVID-19 treatment per the CARES Act. If you are uninsured, the Provider Relief Fund could reimburse providers for treatment but that is up to the provider to apply for it, otherwise, you may be liable for the bill.
The LA Times reported a situation where COVID-19 treatment became a huge financial burden ($42,000 in out-of-pocket) because the individual had a grandfathered self-insured plan which does not have an out-of-pocket maximum limit (grandfathered plans do not have to comply with the Affordable Care Act/Obamacare out-of-pocket maximum limit elimination and self-insured plans are not subject to the same federal regulations). The article compared how another person with a similar total cost of care but an out-of-pocket maximum limit ended up with out-of-pockets costs around $1,000.
The American Health Insurance Plans (AHIP) has compiled an inventory of what insurers are doing in response to the pandemic (visited March 1st, 2021). Here are the highlights from the five major insurers on COVID-19 treatment cost-sharing (deductibles, co-pay, co-insurance) or out-of-pocket costs. They are essentially are waiving cost-sharing but the date ranges and extensions vary.
Aetna previously waived cost-sharing for inpatient admission treatment for COVID-19 (announced September 23rd, 2020 and effective until December 31st, 2020 for Commercial and Medicare Advantage.
United Healthcare has extended its COVID-19 treatment cost-sharing waiver for Individual and Group during the month of January 2021, and for Medicare Advantage there is no cost-sharing until March 31st, 2021.
Cigna is waiving cost-sharing for COVID-19 treatments until February 15, 2021, but that is only mentioned on the AHIP website and not date-stamped on Cigna’s website itself.
Humana is waiving cost-sharing for COVID-19 treatment for all lines of business (Commercial, Medicare Advantage and Supplement, Medicaid) with not definite expiration date.
Anthem has extended its COVID-19 treatment cost-sharing waiver until of January 31, 2021.
Your health insurance should cover the cost of COVID-19 testing and any related services, but an out-of-network provider or lab could be charging your insurer higher than usual fees
If you’re uninsured, there may be state (Medicaid) or commercial (brand awareness) entities that are offering free tests, otherwise you have to pay the cash price
A COVID-19 diagnostic test that costs $100 is a reasonable rate (as of 2021, Medicare pays this amount for a test result within two days, otherwise $75). The rates are different for antigen and antibody tests.
More affordable ($30) and convenient options (results via app), such as at-home kits are forthcoming
—
If you’ve been watching traditional news on television or the internet, my bet is that you were told that COVID-19 tests are free. That is true for the most part because the Families First Coronavirus Response Act(passed on March 18, 2020) stipulates that all COVID-19 testing should have no cost-sharing, including deductibles, co-insurance and co-pay for the duration of the COVID-19 public health emergency (since January 27, 2020 and last renewed for another 90 days on January 21, 2021). Costs include the vaccination, administration and any related services and is relevant to private insurance, Medicare, Medicaid and other government programs, for defense, veterans and Native Americans. Medicaid may choose to cover uninsured individuals (receiving reimbursement via 100% Federal Medical Assistance Percentage).
The CARES Act passed on March 27, 2020 further stipulates the all COVID-19 diagnostics tests must be covered as long as they have been or intend to undergo review for emergency authorization use or is authorized directly by the Department of Health and Human Services. Private health plans would reimburse the negotiated rate, if not negotiate one or pay the cash price listed publicly on the website (a provider can face penalties for not listing the cash price). The tests will also be covered as preventative services within fifteen days and not the customary one year based on the recommendations of the authority bodies (USPTF or ACIP).
The Peterson-KFF (Kaiser Family Foundation) Health System Tracker (published July 15, 2020) found cases where patients do end up with bills or health insurers paying much higher prices than usual for both diagnostic and antibody tests (CDC references for the difference between these two types tests). The Advisory Board published a brief on June 17, 2020 that conveys how providers or labs for COVID-19 diagnostic testing are taking advantage of out-of-network cash prices that are well above the Medicare reimbursement rate of $100. They both point out that higher costs paid by the insurer can lead to higher future premiums to the detriment of the consumer.
More recently, Bloomberg (published on December 15, 2020) mentioned how the FDA approved an at-home test that could cost $30. After returning to the lab, it takes fifteen minutes to deliver results via an app. The mechanism for testing is a nasal swab and could be less accurate – it detects proteins on the virus’ surface (antigen), not the virus’ genetic makeup (diagnostic).
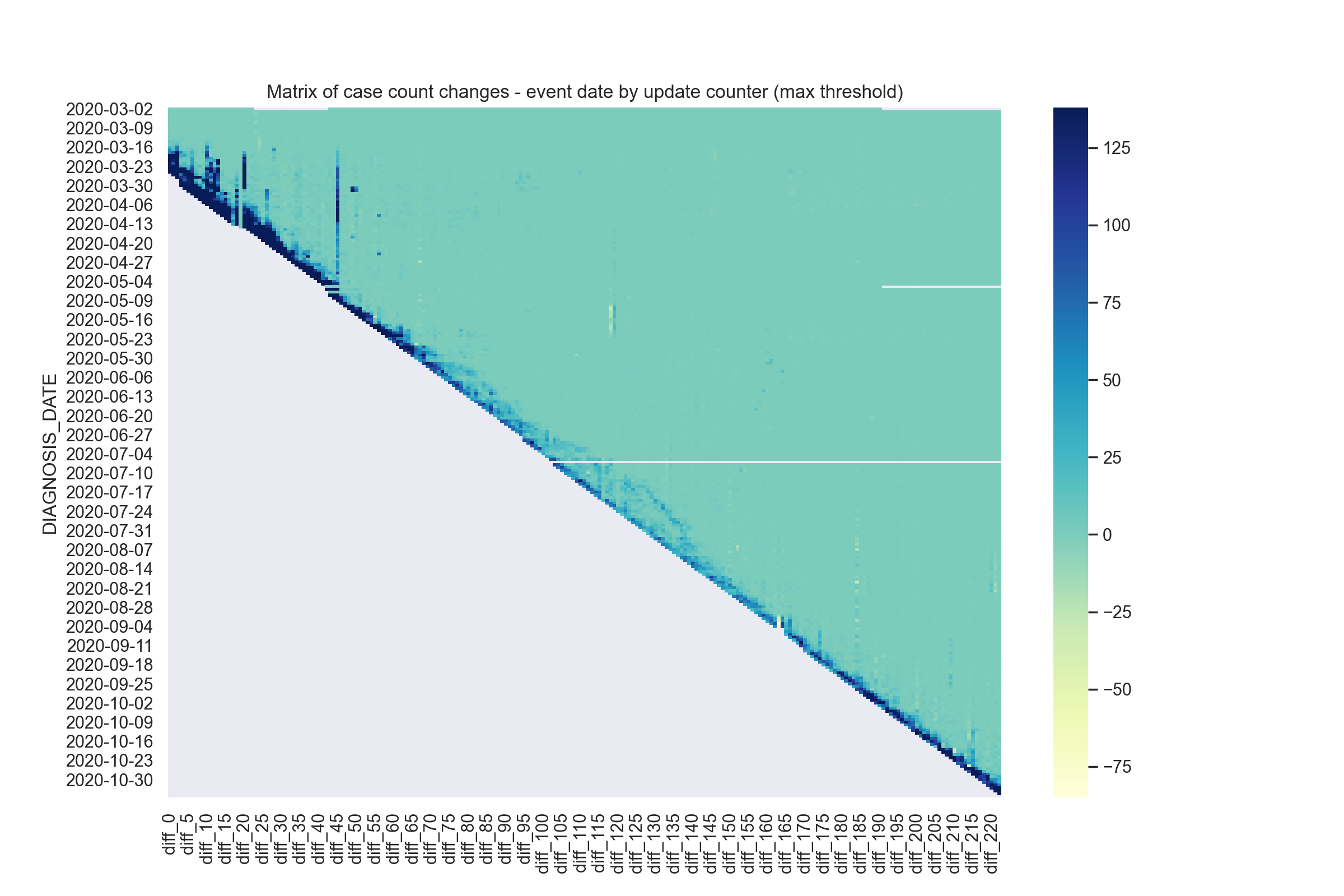
There is significant lag in reporting diagnosis date of COVID-19 cases in New York City by days, sometimes weeks or much further back (mostly in the beginning)
Case counts by diagnosis date follow a weekly pattern, likely mirroring testing availability
—
When COVID-19 first came to America, I would monitor the New York City case count daily to help me make a short-term decision as to how frequently I should be going out. I also tracked the numbers to predict when it would likely taper down so that I can prepare myself psychologically to be physically isolated for an extended period of time. New York City does a good job of making the data accessible and I wanted to know retrospectively whether my decisions of going out of my home were good.
I extracted data from their github repository and downloaded all prior data versions. They changed their folder and data schema a few times, so for this first analysis, I took the easiest route and got around the first six months of data. I did a simple analysis of only the case count and thought about the data in three ways. The first is a matrix showing the case count change after each update by event date. The other two are the cumulative case count changes by event date and update iteration, respectively. So how skewed are the numbers from what they actually tallied up towards? And going into the fall, was the tallying closer to what the numbers actually ended up as?
In the first few months (March to May), there were significant retrospective updates across earlier diagnosis dates, sometimes with the addition of over two thousand cases. During May, there was one massive retrospective update that backdated cases all the way to March. As we approached the summer, the additional retrospective case counts continued to occur up to around a week but at a significantly lower magnitude. Approaching the fall in September and October, there was a continued lag but it spanned a shorter backdate range than previously. However, as cases started increasing again, the number of cases being backdated was higher than the summer.
If we look at the case count by event date, we will notice the weekly pattern that possibly follows the availability of testing.
That pattern does becomes less clear when we look by update counter (updates generally occur daily).